


We’re kicking off this month’s newsletter with an announcement of an important milestone: for the first time, 12 U.S. states, from Colorado to Vermont, have officially proclaimed September as Perimenopause Awareness Month, thanks to a joint effort by the National Menopause Foundation and Perry. It’s a beautiful step toward raising visibility for one of the most under-recognized and undertreated life stages. If this month’s headlines highlight anything, it’s that menopause is getting the attention it deserves.
Perimenopause and menopause are not just hormonal changes: they mark a life transition. This transition carries profound impact for chronic health, mortality risk, and long-term quality of life, while also shaping women’s day-to-day experience of care and wellbeing.
TL;DR
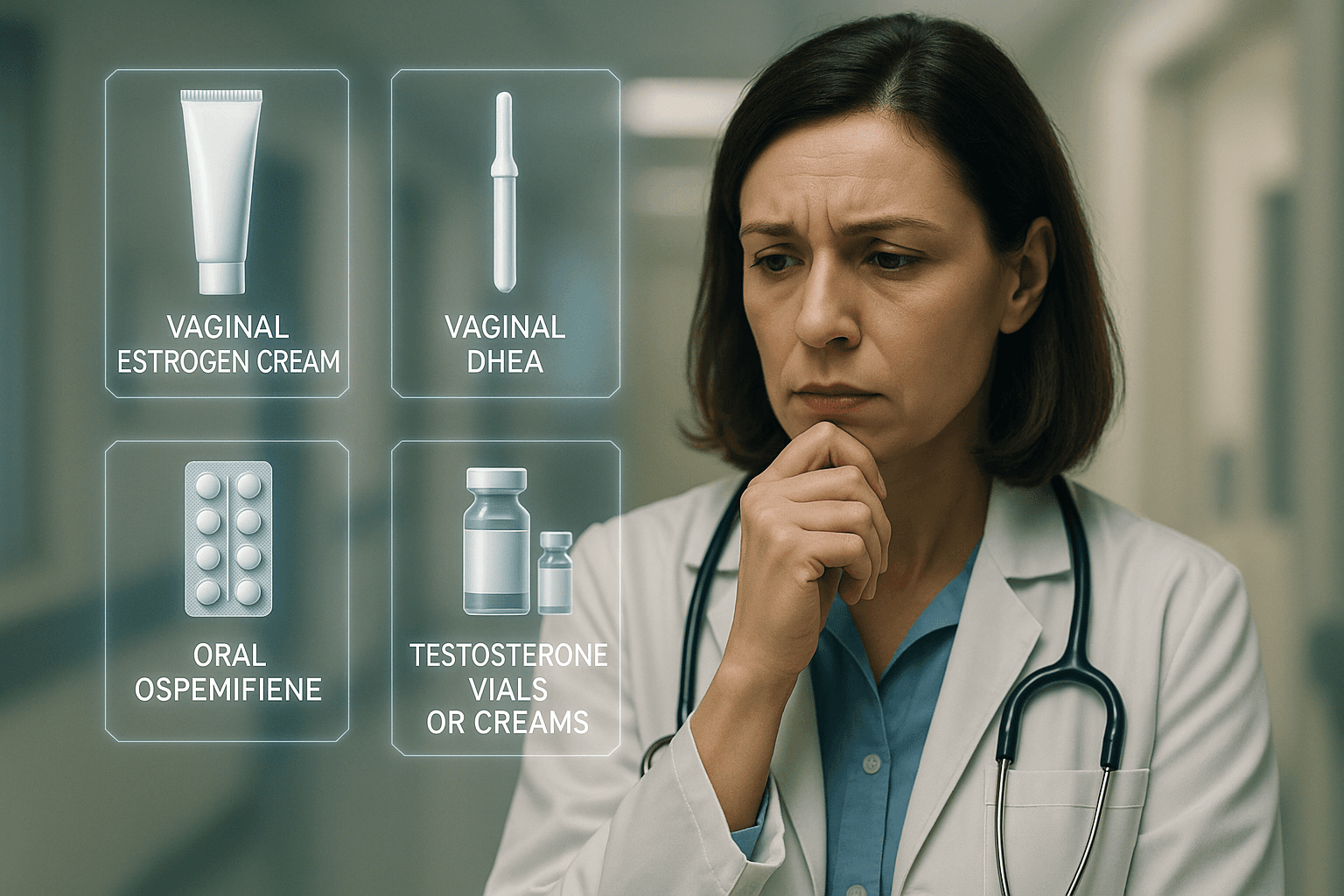
✔️ GSM guidelines: The AUA/SUFU/AUGS guideline strongly supports local low-dose vaginal estrogen as first-line therapy, with conditional roles for vaginal DHEA and ospemifene. Energy-based devices, testosterone, and oxytocin lack evidence however.
✔️ Menopause and Multiple Sclerosis (MS): New ECTRIMS data show early research suggesting menopause status shapes initial MS presentation and comorbidity burden.
✔️ Weight, HRT, and GLP-1s: WeightWatchers’ new menopause programme is backed by early internal evidence, but could the commercial narrative risk override where the research currently stands?
GSM guidelines: what works vs what doesn’t.
The AUA/SUFU/AUGS has refreshed the guidelines for genitourinary syndrome of menopause (GSM), based on an AHRQ/PCORI-funded systematic review. The take-home message is clear: (1) diagnose clinically, (2) treat what matters to the patient, and (3) be cautious with options that create an illusion of validity but lack quality evidence.
GSM is a clinical construct encompassing vulvovaginal, urinary, and sexual symptoms associated with estrogen/androgen decline, but there is still no consensus on how many or which symptoms are required for diagnosis. The systematic review graded interventions against COMMA outcomes (e.g., pain with sex, dryness, dysuria, Most Bothersome Symptom [MBS], quality of life, satisfaction, side effects) using GRADE (a systematic approach assessing evidence certainty and strength of recommendations in healthcare guidelines).
What actually works, and how confident are we?
Local low-dose vaginal estrogen improves vulvovaginal discomfort/irritation, dryness, and dyspareunia with reassured safety. It is also recommended for women with recurrent UTIs to reduce future infections, with no clearly superior route of administration. This leaves the choice to shared decision-making around preferences, dexterity, anatomy, and access. In patients already on systemic estrogen who still have GSM symptoms, adding local low-dose vaginal estrogen (or vaginal DHEA) is appropriate. Furthermore, local low-dose vaginal estrogen may improve genitourinary symptoms in the presence of comorbid overactive bladder complications as well.
✔️ Strong recommendation; Grade C evidence and Expert Opinion.
Vaginal DHEA may improve dryness, dyspareunia, and quality of life, but has been associated with slightly higher rates of adverse events (e.g., discharge and flushing). Short-term trials show acceptable endometrial safety, but the safety of systemic DHEA remains uncertain.
✔️ Moderate recommendation; Grade C.
Oral ospemifene may improve dryness and dyspareunia, with higher treatment satisfaction, particularly when patients prefer oral therapy or cannot use vaginal products. However, marginal increases in hot flushes, discharge, and candidiasis have been observed.
✔️ Conditional recommendation; Grade C.
Options not recommended outside research settings include?
Energy-based therapies (CO₂/Er:YAG laser)
❌ Claims to stimulate collagen formation, angiogenesis, and epithelial thickening have not demonstrated efficacy compared to sham or estrogen for COMMA outcomes. The broader evidence lacks robust long-term harm data and is confounded; therefore, these devices are not supported for GSM symptom relief.
Vaginal/systemic testosterone and vaginal oxytocin
❌ Small, low-quality trials suggest possible benefit of vaginal testosterone for sexual function and dyspareunia, but evidence is too limited, imprecise, and inconsistent to recommend for GSM (according to the AHRQ/PCORI-funded systematic review). Vaginal oxytocin is not commercially available in the U.S. (compounding only) and likewise lacks sufficient evidence for GSM.
In the included trials, when treatment was effective, symptom improvement generally began within 1–2 months and continued through about 12 weeks in trials. However, the trials were underpowered to detect rare adverse events, and side-effect profiles varied by therapy, necessitating continued safety and efficacy data on hormone therapies for GSM.
Phenotyping MS using menopause status?
In this month, researchers at the European Committee for Treatment and Research in Multiple Sclerosis, Yasemin Şimşek and colleagues, shared novel findings that menopause may shape how multiple sclerosis (MS) first presents in women, and what comorbidities they are most likely to face.
In premenopausal women, MS more often began with optic neuritis (21.8%), whereas spinal cord onset was most common in postmenopausal women (44%) and men (48.3%). Şimşek suggested that estrogen-driven inflammatory responses may underpin optic neuritis in premenopausal women, while declining hormonal protection and age-related neurodegeneration shift the presentations toward the spinal cord later in life.
Moreover, postmenopausal women showed higher rates of cardiovascular (24.7%) and metabolic disorders (10.3%), while premenopausal women more frequently experienced psychiatric conditions, such as depression and anxiety.
What does this mean for your practice today?
✔️ MS presentation varies by life stages. Menopause status is a key biological inflection point that influences both initial symptoms and long-term comorbidity risk.
✔️ Men and postmenopausal women may require a stronger emphasis on neuroprotection/disability prevention and cardiovascular risk management.
✔️ Premenopausal women may benefit from closer relapse monitoring and DMT optimization with proactive screening and support for mood and anxiety symptoms.
⚠️ The evidence remains early-stage and not peer-reviewed. As such, guidelines have not changed, but this study highlights a critical step towards MS phenotyping and precision management by accounting for sex and hormone stage.
WeightWatchers: from diet culture to midlife care?
For decades, WeightWatchers has been praised for helping millions lose weight and build community, but also criticised for perpetuating yo-yo dieting, scale obsession, and the commercialization of body image. This month, the company announced WeightWatchers for Menopause, a programme bundling nutrition guidance, fitness coaching, peer community, and access to HRT, GLP-1 receptor agonist medications, and other evidence-based interventions when clinically appropriate.
WeightWatchers cites internal data suggesting that women of menopausal age who followed its programme lost nearly four times more weight than those managing independently using standard nutritional guidelines. Whether conditions between groups were fully matched is unclear.
Nonetheless, at ENDO 2025, Mayo Clinic investigators reported greater weight reduction with tirzepatide plus menopause hormone therapy than with tirzepatide alone (about 17% vs 14% average total body-weight loss over ~18 months), emphasizing earlier findings with semaglutide plus hormone therapy use. These results suggest a combination benefit for postmenopausal women, but confirmation in larger, longitudinal, prospective cohorts is still pending to assess generalizable long-term efficacy, adherence, and safety.
Crucially, prescribing HRT or GLP-1 agonists should follow a personalised risk–benefit assessment and shared decision-making.
That means:
✔️ Screening for contraindications
✔️ Reviewing concurrent medications and comorbidities, access and cost, and patient goals.
✔️ Setting monitoring plans via self-reported symptom relief, blood parameters, strength and function, advanced imaging techniques, and adverse effects, to name a few.
✔️ Providing frequent follow-ups for dose adjustments, discontinuation, or switches if risks outweigh benefits.
It’s striking how quickly mainstream weight-loss brands are moving into the menopause space. Commercial narratives can outpace evidence for symptom control, cardiometabolic risk reduction, and long-term adherence, but perhaps WeightWatchers is aiming to redeem its reputation by introducing more stringent evidence and clinical backing into its programs, where appropriate. Ultimately, there’s much more to learn about their processes as details emerge.
Many patients will benefit from integrated care, and the challenge is distinguishing marketing claims from evidence-based practice. That’s why, at Dama, we’re building tools and integrations that help clinicians, like you, stay current with the latest evidence, especially where research is still evolving. That’s how we strive to keep care patient-centred and genuinely personalized.
Our focus.
At Dama Health, we are continuing to build infrastructure and integrations that adapt to your clinics with robust medical and clinical backing.
We are also now offering fully customised lead-generation & conversion quizzes designed for your practice, so that more women who visit your website feel recognised, understood, and guided to the right care. For you, this means higher patient conversion, and for them, it means the reassurance of being acknowledged and cared for by the level of support and personalisation you bring into the clinic. If you're interested, feel free to reply with a simple "YES."
That's it for now! We're excited to be back in a month's time with new insights in the precision and women's hormone health space.
Best,
The Dama Health Team