


Last month, we opened our newsletter with a pivotal announcement in relation to the FDA’s decision to remove the long-standing black box warning from estrogen therapies. This month, we find ourselves confronting concerns from the scientific community about the decision-making process and the evidence behind the claims made during the FDA webinar. The field is moving fast, and careful interpretation of evidence and thoughtful clinical implementation matter more than ever.
So, here's what stood out in November:
✔️ Black box debate: The FDA removed long-standing black-box warnings from estrogen-containing therapies, a decision widely welcomed across women’s health. However, criticism emerged focused on how the decision was made, including concerns about the evidence and claims presented during the FDA’s webinar.
✔️ PCOS phenotyping enters the data-driven era: A 47,000-participant analysis identifies four reproducible PCOS subtypes with distinct metabolic profiles and reproductive trajectories. It’s a significant step toward structured risk stratification, particularly in fertility optimization settings.
Concerns about the removal of the black box warning on estrogen.
The FDA’s recent removal of the boxed warning from estrogen-only hormone therapy marks a meaningful milestone. A boxed warning is the strongest caution the agency issues, typically reserved for drugs with clear, significant, and severe risks. For years, menopause experts have argued that this designation was inappropriate and stemmed from outdated interpretations of early WHI findings. From this standpoint, removing the boxed warning represents a positive and long-overdue correction that better aligns the labeling with the latest evidence and re-evaluation of the WHI study.
What the pushback is actually about:
Much of the pushback from researchers and clinicians has not been about reinstating the boxed warning, but rather about how the decision was made and how the evidence was communicated.
1. Traditionally, label changes follow a rigorous, transparent pathway that includes advisory committee reviews, public evidence review, and broad scientific consultation. In contrast, this ruling emerged from a short-format roundtable, closed to prior public discussion. The FDA defended the new approach as an alternative to “bureaucratic, long, often conflicted and very expensive” advisory meetings. Whether this format preserved the scientific process and credibility remains uncertain.
2. Many experts expressed concern that the FDA’s update relied on a limited set of older studies and did not clearly articulate the latest evidence to support the change. The FDA x JAMA press release leaned on three dated, low-quality publications, which experts suggest were cherry-picked and chosen largely for their dramatic results:
a 45-year-old case-control study on fractures relying only on self-reported estrogen use;
a 34-year-old narrative review on unopposed estrogen and cardiovascular disease, built on one 1979 clinical trial and several low-quality observational studies;
a 29-year-old retrospective case-control study linking estrogen use to reduced Alzheimer’s mortality, based on a small, community-specific cohort with no pharmacy validation and no data on progestogens.
These were not randomized trials and could not establish causality. The findings were also influenced by socioeconomic status, education, and healthy-user bias. The concern is that without clear communication about the evidence, its gaps, and limitations, the decision may be misinterpreted by the public and by some telehealth providers. This could accelerate a trend toward positioning systemic estrogen as a “longevity drug” or prescribing it without evaluation of risk and benefit: cardiovascular risk, cancer history, comorbidities, or timing of initiation, areas where nuance truly matters.
So what does the evidence actually say?
Based on large studies like RCTs and meta-analyses from recent years, current data do not show that systemic HRT prevents cardiovascular disease, dementia, or premature death. Modern formulations may ultimately show better outcomes, but the high-quality RCT evidence needed to make preventive claims simply does not exist yet. This is why conventional guidelines do not recommend HRT as a preventive therapy (except for osteoporosis), but rather as a highly effective treatment for menopause symptoms.
What this means for your practice:
✔️ Do not be afraid to prescribe HRT when clinically indicated.
Many women who should be offered hormone therapy still are not receiving it. The removal of the boxed warning is a positive correction and should empower evidence-aligned prescribing.
✔️ The concern is not about HRT itself, but about communication and process.
Clinicians have raised valid questions about the transparency, evidentiary basis, and communication around the update, not about whether HRT “should” be prescribed.
✔️ We urgently need high-quality real-world data on modern HRT regimens.
Most past trials used older formulations. There is a major opportunity and responsibility for clinicians to help generate modern, diverse RWD on outcomes, safety, and patient-reported experience.
Data-driven PCOS Subtypes: clarifying metabolic risk and reproductive outcomes
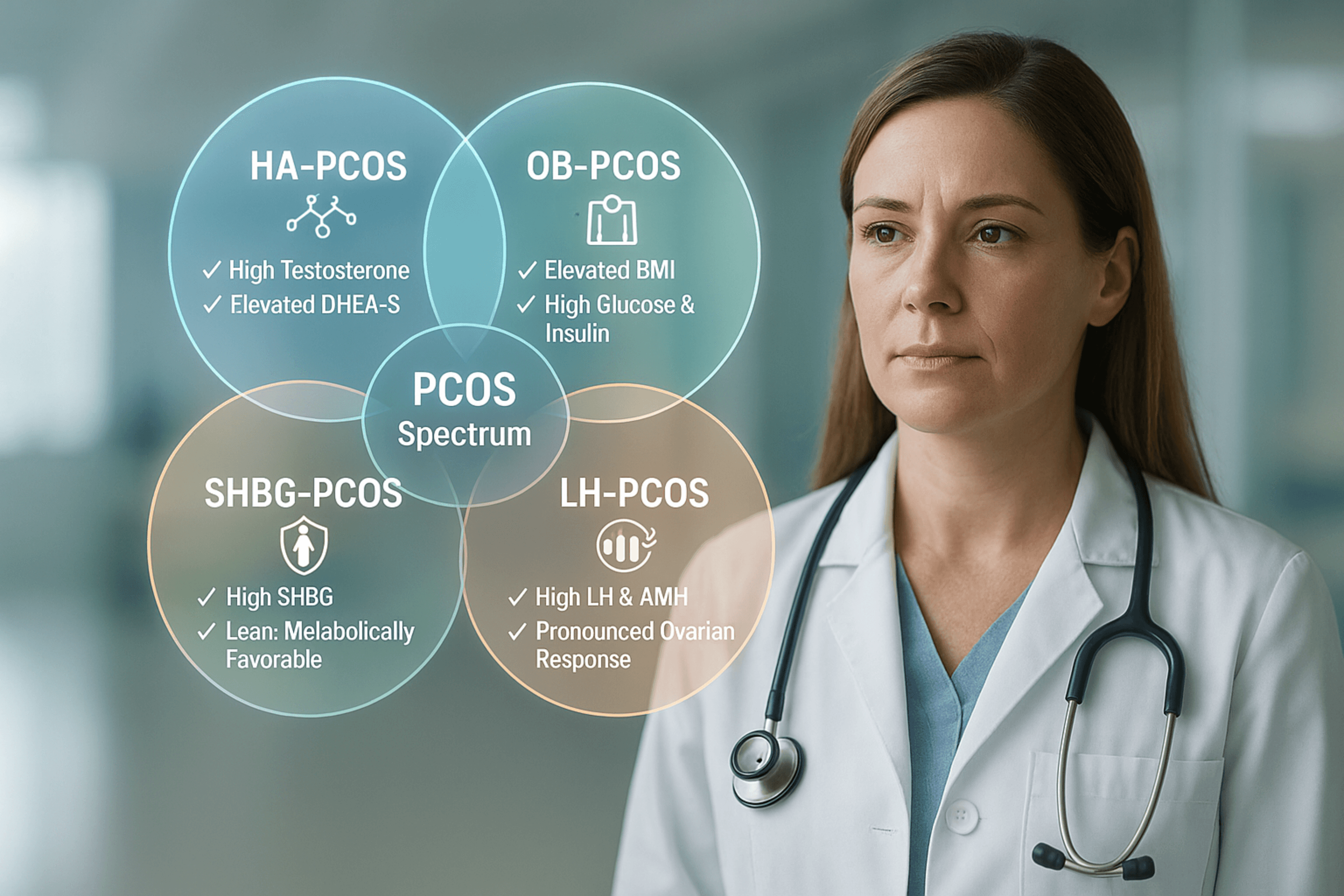
A recent large multicentre analysis offered fresh insight into the heterogeneity of polycystic ovary syndrome. Drawing on data from more than 47,000 women, researchers used nine routine biomarkers, such as BMI, LH, FSH, testosterone, SHBG, DHEA-S, AMH, fasting glucose, and fasting insulin, to see whether distinct metabolic or reproductive trajectories emerge over time, and whether these phenotypes influence long-term health.
Among 11,908 untreated women in the discovery cohort, four distinct subtypes appeared and were validated across five international datasets (see image below).
The question was simple but important: Do these patterns predict different health trajectories over time?
Across approximately 6.5 years of follow-up, the groups reflected distinct metabolic and reproductive trajectories.
1. OB-PCOS
The OB-PCOS subtype carried the highest risk of type 2 diabetes, MASLD, and hypertension, likely explained by pronounced insulin resistance and broad metabolic dysfunction. As a result, reproductive abnormalities appear secondary to this metabolic burden
2. LH-PCOS
Women in this group had the lowest odds of spontaneous remission. Elevated LH and strikingly high AMH suggest a large follicle pool and heightened ovarian responsiveness, which may explain both persistent PCOS features and a greater tendency toward ovarian hyperstimulation during fertility treatment.
3. HA-PCOS
This hyperandrogenic group showed marked dyslipidaemia and the highest rates of second-trimester loss and premature rupture of membranes. The authors suggest androgen-driven effects on hepatic lipid metabolism and impaired endometrial receptivity and placentation.
4. SHBG-PCOS
With higher SHBG and consequently lower free-androgen exposure, this subtype had the most favorable metabolic profile and the lowest long-term cardiometabolic risk. Reproductive dysfunction was also comparatively mild.
Nonetheless, the 2025 study presents some limitations.
The study provides a helpful organizing framework, but several limitations matter for everyday practice:
Key clinical symptoms, such as menstrual regularity, were not included, which may limit real-world applicability.
Follow-up relied on self-report via telephone, and the ultrasound data used outdated follicle thresholds (≥12 follicles), which may have affected diagnostic accuracy.
Most women recruited were undergoing fertility treatment, and the model did not include genetic or molecular markers, limiting generalizability to the broader PCOS population.
What this means for your practice:
✔️ The four subtypes can help you anticipate metabolic risk, ovarian response, and potential pregnancy complications. They offer a clearer language for describing the heterogeneity that many clinicians and experts observe in practice.
✔️ But, they’re not ready to replace clinical judgment. PCOS almost certainly exists along a continuum, as many patients will present overlapping biochemical profiles. The model may also be less applicable to adolescents, community-diagnosed patients, women not seeking conception, or diverse ethnic groups.
This research moves us toward a more nuanced understanding of PCOS, but it does not yet warrant changes to care pathways. For now, these subtypes are best used as a lens for discussing risk and guiding individualized care.
Warmly,
The Dama Health Team