


Hi everyone,
As midlife women’s health continues to advance, we are finally seeing outdated clinical principles disappear in favor of more nuanced, equitable, and whole-patient care.
In this month’s issue, we’re bridging the gap between new clinical evidence and your day-to-day workflow. We’ve curated the most practice-changing updates and tools you need to know about this month:
✔️ The End of PCOS: Why the 90-year-old diagnosis has officially been replaced by PMOS, and how this “metabolic” reclassification will change your GLP-1 prescribing.
✔️ ACOG’s PMB Update: Why relying on a ≤4mm ultrasound stripe to rule out endometrial cancer is no longer the standard of care for high-risk patients.
✔️ Building Your AI Stack: Cutting through the tech noise to identify why actually belongs in a 2026 women’s health clinic.
✔️ A free Clinical Tool: Our interactive MHT Dose Switcher helps you navigate patch shortages and formulation changes in seconds.
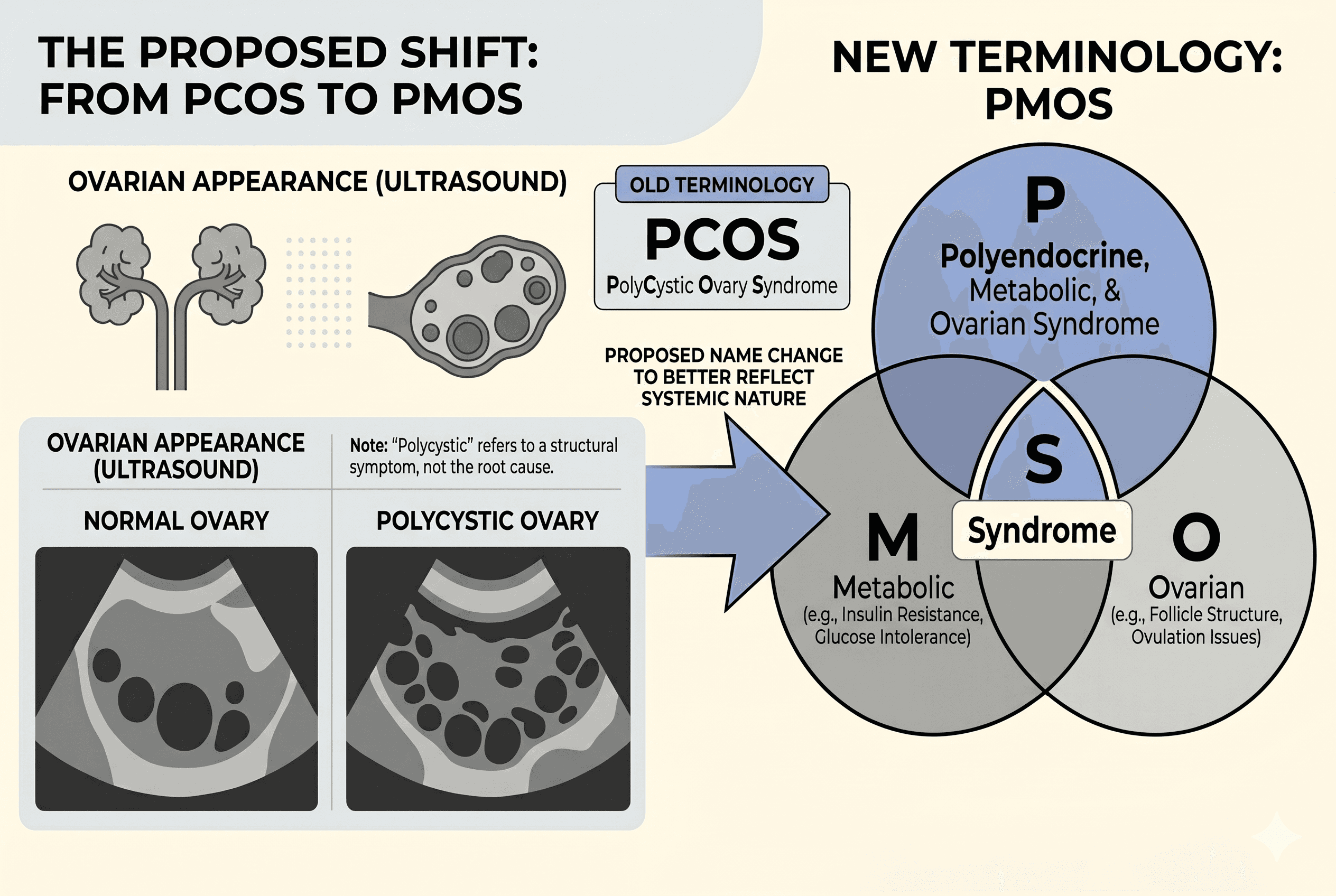
Goodbye PCOS. Hello PMOS:
We’ve all had this exhausting conversation: trying to explain to a frustrated patient why her pelvic ultrasound is perfectly "clear," yet she still has PCOS.First recognized 91 years ago and named in 1990 to diagnose the presence of “both ovulatory dysfunction and clinical hyperandrogenism and/or hyperandrogenemia,” PCOS has been renamed to Polyendocrine Metabolic Ovarian Syndrome (PMOS), after a 97% consensus across 56 medical organizations over 14 years of global collaboration.
The pre-name, PCOS, was originally coined to diagnose the presence of excess small antral follicles (sacs that house immature eggs), however, the general misperception among clinicians and women biased the presence of pathological, in particular, ovarian cysts as a defining feature of the condition, leading to “delayed diagnosis, fragmented care, and stigma.” These faults led to repeated disruptions in clinician-patient relationships and distrust in the medical system. This was evidenced in a global survey of 7,000 respondents in which “85% of patients and 62% of clinicians associated PCOS with ovarian cysts.”
Instead of having to explain to a frustrated patient why her ultrasound is "clear" but she still has PCOS, now, PMOS requires systemic reframing of PCOS as a sole gynecological condition and officially classifies this as a lifelong, multisystem metabolic condition:
Polyendocrine: Validates that the primary drivers are complex hormonal imbalances (elevated androgens, LH).
Metabolic: Centers the highest-risk morbidity factors: insulin resistance, type 2 diabetes, and cardiovascular risk.
Ovarian: Acknowledges the downstream effects on anovulation and fertility (antral follicles, not cysts).
Reflecting the multi-systemic nature of PMOS, researchers currently recognize four endotypes: hyperandrogenic (HA-PCOS), overweight-obesity, high SHBG, and elevated LH and AMH. As such, the name change opens access to better insurance coding and out-of-pocket coverage for metabolic therapies, such as GLP-1s, that were previously denied as "fertility treatments." For example, for women with the overweight-obesity endotype, GLP-1 receptor agonist therapy has been shown to be a potent insulin resistance, hyperandrogenism, weight management, and inflammation mediator, alleviating menstrual irregularities and ovulatory irregularities. Although GLP-1s are not currently covered for PCOS, by insurance, the broadened metabolic scope of the condition allows for greater recognition of weight management in many women with PMOS.
Clinical Takeaways:
✔️ Leverage the official addition of the word Metabolic to the condition name to provide a stronger clinical and coding rationale for using GLP-1 receptor agonists and other metabolic agents for PCOS as a means of targeting the root systemic drivers of PMOS, rather than just downstream reproductive symptoms
✔️ With the name change removing the barrier to falsely associating PMOS with pathological cysts, “clear” pelvic ultrasounds in the presence of PMOS can be explained that the “ovarian” term refers to ovulatory dysfunction driven by a neuroendocrine imbalance.
✔️ Ensure that you update EMR macros, smart phrases, and superbills to reflect PMOS and avoid billing rejections, ensuring proper risk-stratification for metabolic morbidities.
✔️ As a lifelong multisystem cardiometabolic condition, lipids, A1C, and blood pressure for these patients will require monitoring well past their reproductive years and through their menopausal transition.
✔️ Clinical Takeaway: Although prospective trials and meta-analyses are limited at this stage, this narrative review suggests that menopausal status and MHT formulations belong in your differential reasoning if a midlife woman presents with new-onset asthma, unexplained chronic cough, atypical anaphylaxis, or suddenly becomes "allergic" to multiple unrelated medications.
ACOG's 2026 Shift: Why a <4mm Endometrial Stripe is No Longer a Guarantee.
With 90% of women with endometrial cancer presenting with vaginal bleeding, and endometrial cancer incidence rates increasing steadily in the United States, ACOG has updated its guidelines to prioritize prompt diagnosis and minimize missed cancers.Historically, the protocol used transvaginal ultrasound (TVUS) as the primary triage tool, deferring biopsy if endometrial thickness was 4mm or less. These guidelines were based on a 99% negative predictive value for endometrial cancer in patients with an endometrial thickness of 4mm or less. However, that figure was built on older prevalence estimates that no longer reflect current cancer rates, and relying solely on this measurement exposes a dangerous clinical gap.
In reality, 5-12% of endometrial cancers are misdiagnosed on initial evaluation because ultrasound detection of endometrial thickness is poorly sensitive for premalignant and malignant pathology. Furthermore, anatomical barriers, such as an axial uterus, obesity, coexisting myomas, adenomyosis, or previous uterine surgery, can all produce an unreliable TVUS result of both endometrial thickness and texture. Furthermore, this detection gap disproportionately harms non-Hispanic Black women, who are at a significantly higher risk for aggressive endometrial cancers that frequently do not present with demonstrable ultrasound abnormalities.
Now, ACOG's 2026 update recommends that transvaginal ultrasonography and endometrial tissue sampling are now part of the initial evaluation for most patients presenting with postmenopausal bleeding (PMB). TVUS-only applies only when all four of the following conditions are simultaneously met:
A single episode of PMB
A sonographically fully visualized endometrium of 4mm or less
Low risk of factors strongly associated with increased endometrial cancer risk (advanced age, obesity, unopposed estrogen use, type 2 diabetes, PCOS/PMOS, atypical glandular cells on cervical cytology, or family history of gynecologic malignancy)
A patient who has been counseled that any recurrent or continued bleeding requires immediate re-evaluation and has no significant barriers to prompt follow-up care.
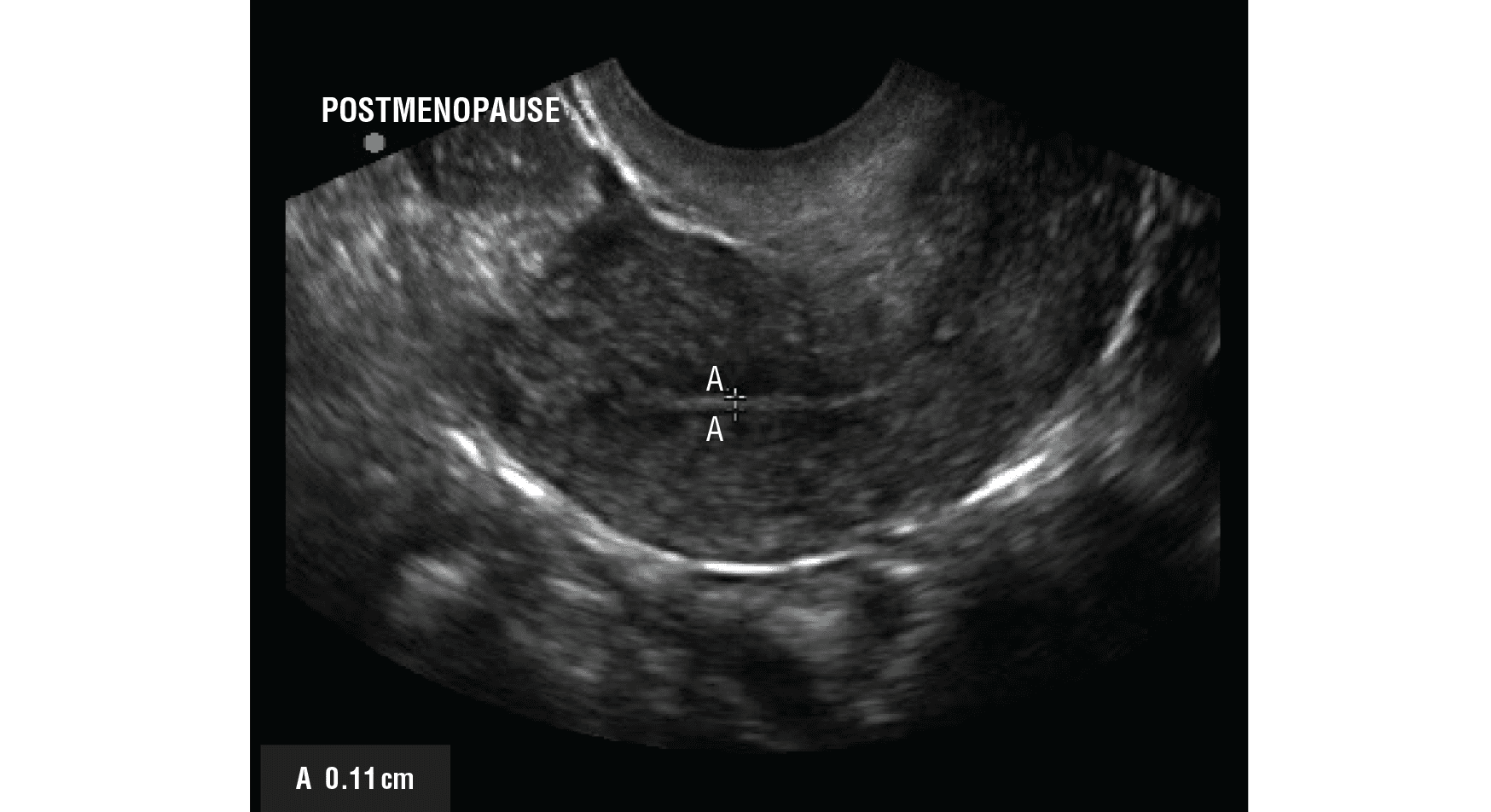
Figure 1. Measurement of endometrial thickness. The endometrial thickness measured at its thickest portion as the distance between the calipers perpendicular to the midline longitudinal plane in the uterus.
What this means for your practice.
✔️ Biopsy is now the default at the first visit: For most patients presenting with PMB, plan for endometrial tissue sampling at the initial diagnostic visit. In-office endometrial sampling, sonohysterography, or office hysteroscopy are all appropriate depending on clinical context. Do not wait for a reassuring ultrasound before proceeding.
✔️ Reserve ultrasound-only triage for the lowest-risk phenotype: TVUS without biopsy is now only acceptable when all four criteria above are met simultaneously. If your patient has even one compounding risk factor, including high BMI, diabetes, exogenous estrogen or SERM use, or is Black, the dual approach is required. (Note: if initial tissue sampling was insufficient for diagnosis, further evaluation is still required.).
✔️ Counsel explicitly on recurrence: Counsel patients that any recurrent or persistent bleeding warrants immediate histologic evaluation (via hysteroscopy with dilation and curettage, for example). Aggressive carcinomas can still present with an endometrial thickness below 3mm.
✔️ A thin stripe does not rule out Type II cancers: A thin endometrial echo does not exclude all possibilities of disease. It does not reliably exclude aggressive Type II endometrial cancers, even at a thickness well below 4mm.
Build Your AI Stack: What Actually Belongs in a Women's Health Clinic in 2026.
There's a lot of noise right now about AI in clinical practice. Every week there's a new tool and a new study. However, whether you're an NP adding perimenopause packages, a functional medicine provider expanding into menopause care, or an OB/GYN scaling your private practice - the tools that exist out there can feel like they were not designed with your workflow and the care you provide in mind.
So what does a useful AI stack for a modern women's health clinic actually look like?
A modern EMR with an integrated AI scribe - your documentation, scheduling and compliance layer. Some EMRs now have scribe functionality integrated, so your notes, your payment system, and your patient record are all in one place. It is worth getting the foundation right to save you frustration and time.
A clinical co-pilot that knows your specialty - this is the gap most clinicians are still patching with a million browser tabs and recall. General AI handles general medicine. For hormone prescribing, you need something that understands the nuance: the evidence base for modern hormone prescribing protocols, the evidence based risk data for complex patients, what the guidelines say versus what current practice supports. This is where Dama Assist comes in - built specifically for hormone care, it helps you work through edge cases, stay on top of latest data and generate evidence-based patient-facing materials. Already trusted by hundreds of clinicians who want to practice with more confidence, speed, and depth. Start your free trial here.
A patient experience layer - digital intake and pre-qualification, automated follow up check-ins, and outcome tracking. This is what separates a clinic that scales from one that plateaus. When your funnel, your follow-ups, and your outcome data are running in the background, you acquire the right patients, get your time back and retain your patients over time. These three layers work together.
Get the tech infrastructure right and the clinical and commercial side of your practice gets easier. If you're ready to take a step toward making your workflows more tech-enabled, innovative, and built for the future - reply to this email or reach out to us at paulina@damahealth.com. We're always happy to help you think through what that looks like for your practice!
The Bottom Line.
If there is a common thread in this month’s updates, it is that women’s health is finally moving past outdated labels and rigid protocols.
Whether it is officially recognizing PMOS as a lifelong metabolic condition, or ACOG acknowledging that a thin ultrasound isn’t a one-size-fits-all guarantee for PMB, or upgrading your clinic's tech stack to include specialty-specific AI, the standard of care is becoming more nuanced, equitable, and whole-patient focused.
At Dama, our goal is to build the tools that help you navigate the point of care without adding to your cognitive load. We hope the new MHT Dose Switcher (completely free!) helps streamline your workflow and save you a few pharmacy call-backs this week. Give it a try at https://checker.damahealth.com/ and let us know what you think.
As always, hit reply if you have any feedback on the new tool or if there are specific clinical topics you’d like us to cover.
See you next month,
The Dama Health Team