


Hi everyone,
This month, we’re diving into the data front of the menopause space. New sleep data from the SLEEP 2026 Annual Meeting suggest a symptom clinicians rarely screen for is doing more damage to quality of life than the ones they traditionally ask about. And two decades after the Women’s Health Initiative (WHI), hormone therapy use is still falling, even in the age band where the evidence clearly shows a favourable risk-to-benefit ratio, an outcome that looks less like a clinical evidence problem and more like a training and confidence gap:
✔️ Sleep disturbance looks like an independent driver of menopausal quality-of-life loss, not just a downstream effect of hot flashes. Women with sleep disruption alone scored lower in health-related quality of life scores than asymptomatic women in a 2,066-woman SWAN analysis, and the decline sharpened when sleep disruption and VMS overlapped (Carina Dinkel-Keuthage et al., 2026).
✔️ Elinzanetant (Lynkuet) reduced objectively measured nighttime wakefulness (WASO) by about 18% more than placebo over 12 weeks in a phase 2 trial (NIRVANA, n=110). A modest but real signal, though it doesn’t quite prove the drug treats sleep disruption independent of VMS (Soares, Joffe and Maki., 2026).
✔️ Systemic hormone therapy use fell from 4.4% to 1.7% of US women 40 and older between 2007 and 2023, even in the age band where risk-to-benefit is most favorable. The gap looks like a clinician training and confidence problem, not a contraindication problem (Faubion et al., 2026).
Hallmark of menopause: Sleep vs Vasomotor Symptoms:
Until now, menopause conversations have centered on hot flashes. Two studies presented at the SLEEP 2026 Annual Meeting argue this emphasis overlooked a key player with regards to quality of life: sleep.
The first study:
Carina Dinkel-Keuthage and colleagues presented a retrospective analysis of 2,066 women from the Study of Women's Health Across the Nation (SWAN). Women were grouped into four symptom groups, based on reportings in the prior two weeks: no symptoms, VMS only, sleep disturbance only, and both VMS and sleep disturbances. The outcomes regarding health-related quality of life (HRQoL) covered physical health limitations, emotional limitations, energy levels, and fatigue.
Women with sleep disturbance alone scored lower on physical HRQoL measures than women with no symptoms (mean difference -3.30; 95% CI, -5.03 to -1.56). VMS alone showed no significant effect on role-physical scores, but when sleep disturbance and VMS occurred together, the drop was largest at 4.76 points (95% CI, -6.45 to -3.07). The same pattern held for energy and fatigue as HRQoL measures. Neither VMS nor sleep disturbance alone had a significant effect, but the two symptoms combined produced a significant drop in energy and fatigue scores by 3.70 points (95% CI, -4.25 to -3.46). On HRQoL measures related to emotions, none of the three groups showed a statistically significant difference from women with neither symptom.
With 40 to 60% of menopausal women reporting sleep disturbance as one of their most bothersome symptoms and objective measures demonstrating hot flashes lengthening time to fall asleep by roughly 6 to 8.5 minutes. On top of effects on sleep quality and number of awakenings, sleep disturbance looks more like an independent driver of quality of life loss, compared to VMS alone (Baker et al., 2018; Law et al., 2026).
Although this analysis relied on single survey items, was self-reported, did not capture severity, and each annual SWAN visit could not describe long term symptom trajectories or intermittent symptoms outside the two-week window, the trial showed considerable evidence in favor of anchoring management to the individual patient.
The second study:
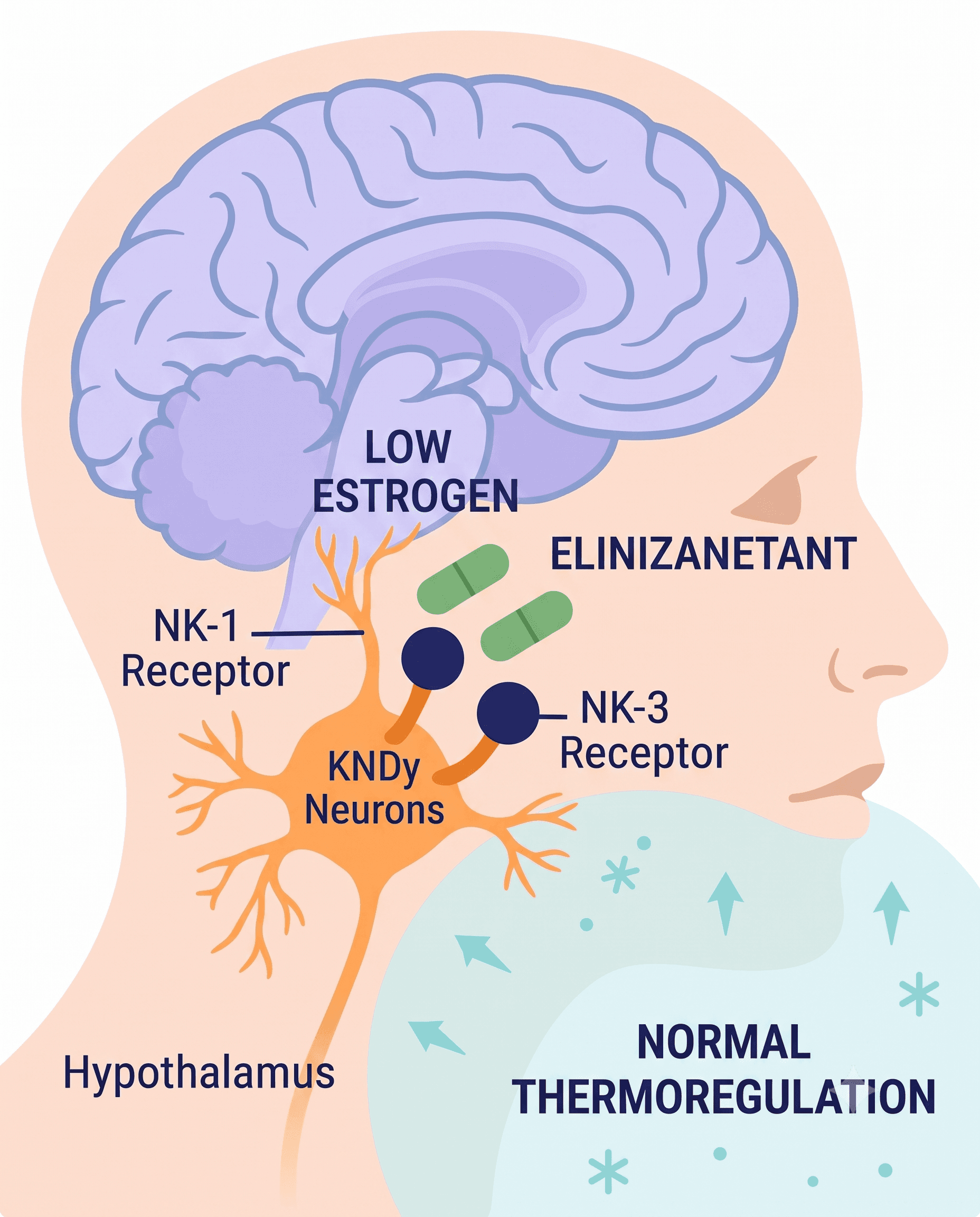
Some of you may recall the FDA’s approval of elinzanetant, a NK3 and NK1 receptor antagonist offering a more direct route to the sleep effect, from a previous newsletter. Its efficacy with sleep was demonstrated through a pivotal OASIS trial. Now, Soares, Joffe, Maki, and colleagues extended this evidence base through NIRVANA, a phase 2 trial using polysomnography (PSG) to objectively confirm sleep disturbance via wakefulness after sleep onset (WASO): the minutes a patient is awake during the night after first falling asleep
110 postmenopausal women with VMS received elinzanetant or placebo for 12 weeks. By week 4, wakefulness at sleep onset (WASO) fell about 32% from baseline with elinzanetant and 6% with placebo, wide enough to determine a clinically meaningful effect. While the advantage narrowed with a relative difference of about 12% at 12 weeks, further analysis on night-to-night variability found an 18% greater reduction with elinzanetant over the full 12 weeks (95% CI, 5 to 30%), translating to about 13 fewer minutes of WASO per night versus placebo. Evidently, the week 4 improvements in sleep outcomes did not persist to the same extent over time, presenting modest results.Nonetheless,this study shows objective consistency with the earlier OASIS data and efficacy of elinzanetant as an adjunct therapy.
Despite modest results, the clinical significance is pertinent. A recent survey from the American Academy of Sleep Medicine concluded that more than a third of (peri)menopausal women report disrupted sleep due to menopausal night sweats or hot flashes. With only 6% of women in that age group reporting no change in their sleep quality during menopause, others reflect sleep disturbance independent of vasomotor events, and will likely not respond to VMS-targeted treatment alone. Here, appropriate patient triaging becomes critical. The neurokinin-targeted drugs, fezolinetant (Veozah) and elinzanetant (Lynkuet), appear to help both symptoms, with elinzanetant's NK1 receptor antagonism offering a more direct route to the sleep effect. That said, the strongest evidence base for managing VMS-independent sleep disruption remains cognitive behavioral therapy for insomnia (CBT-I), as recommended by sleep medicine societies.
Takeaways:
✔️ Tip for the clinic tomorrow: reassess a sleep complaint in a menopausal patient since it may not be a hot flash complaint by another name. Ask whether she wakes because she's hot, or wakes for reasons she can't tie to a hot flash. The answer may guide whether VMS-targeted therapy or CBT-I is the most suitable first line treatment, or whether it’s a combination of both.
✔️ Although VMS-targeted therapy remains a reasonable first-line treatment when hot flashes clearly drive the sleep complaint, elinzanetant's approval is still for VMS, not a sleep treatment. The phase 2 sleep data are encouraging, not definitive, as the effect size is modest.
Have HT use caught up with the growing public awareness of menopause.
Systemic hormone therapy use fell 18% in the decade following the 2002 Women's Health Initiative (WHI) findings. Since the last usage metrics were published in 2007, public awareness around menopause and the safety and efficacy of hormone therapy has accelerated. A Mayo Clinic-led team ran a retrospective analysis of medical and pharmacy claims to track systemic HT use in US women aged 40 and older from 2007 through 2023, across all estrogen-containing hormone therapy formulations and routes of administration options.
Overall systemic HT use fell from 4.4% in 2007 to 1.7% in 2023, even after adjustment for age, race, income, education, and region. That's roughly a 2.5-fold drop in prescriptions lasting at least 180 days, consistent across white, Black, Hispanic, and Asian women. The formulation specifics shifted too: oral conjugated estrogen (CE) prescriptions fell to under 1% of use by 2023, with low-dose oral and transdermal options now more common. Transdermal HT (patches, sprays, gels, creams) declined more modestly than oral HT, likely because oral HT started from a larger base of use to begin with. Even in the age bands where the risk-to-benefit profile is most favorable (within roughly 10 years of menopause onset), use stayed low with less than 4% of women aged 50 to 59 who were recognized as HT users in 2023.

Trends in systemic hormone therapy use among (peri)menopausal women from 2007 to 2023.
A call to action for the noticeable gap in clinician confidence.
Despite declining HT use during this period, this study doesn't capture compounded bioidentical hormone use, which sits outside both FDA approval and pharmacy claims entirely. The study period also runs almost entirely through years when estrogen-containing products, down to low-dose vaginal preparations, carried a boxed warning citing cardiovascular disease, breast cancer, and dementia risk, plus lowest-dose-shortest-duration language that didn't reflect prescribing nuance or the guidelines clinicians were actually working from. Considering these limitations and the removal of the warning late last year in 2025, the prevalence in this study may not reflect current HT use trends and prevalence. Moreover, clinician training hasn’t nearly caught up: .decades of residency programs have offered limited peri/menopause education, even as guidelines increasingly call for individualized symptom management, leaving many clinicians without the training to actually do so. Patients meanwhile, often arrive with hesitation shaped by years or stigma and misinformation around hormone therapy use.
All in all, yes, menopause symptom management should remain individualized but more importantly, this is a call to action for the noticeable gap in clinician confidence around how to assess and triage patients to the right therapy at the right time. At Dama, we are working together with clinicians to narrow the education gap in hormone prescribing by partnering with different groups, including the clinical team at UCHealth’s Women's Integrated Services in Health (WISH), as well as board certified prescribers like Michele Wagner (PharmD, BCPS) to support education efforts with a guard-railed specialist co-pilot tool, Dama Assist, and host webinars.
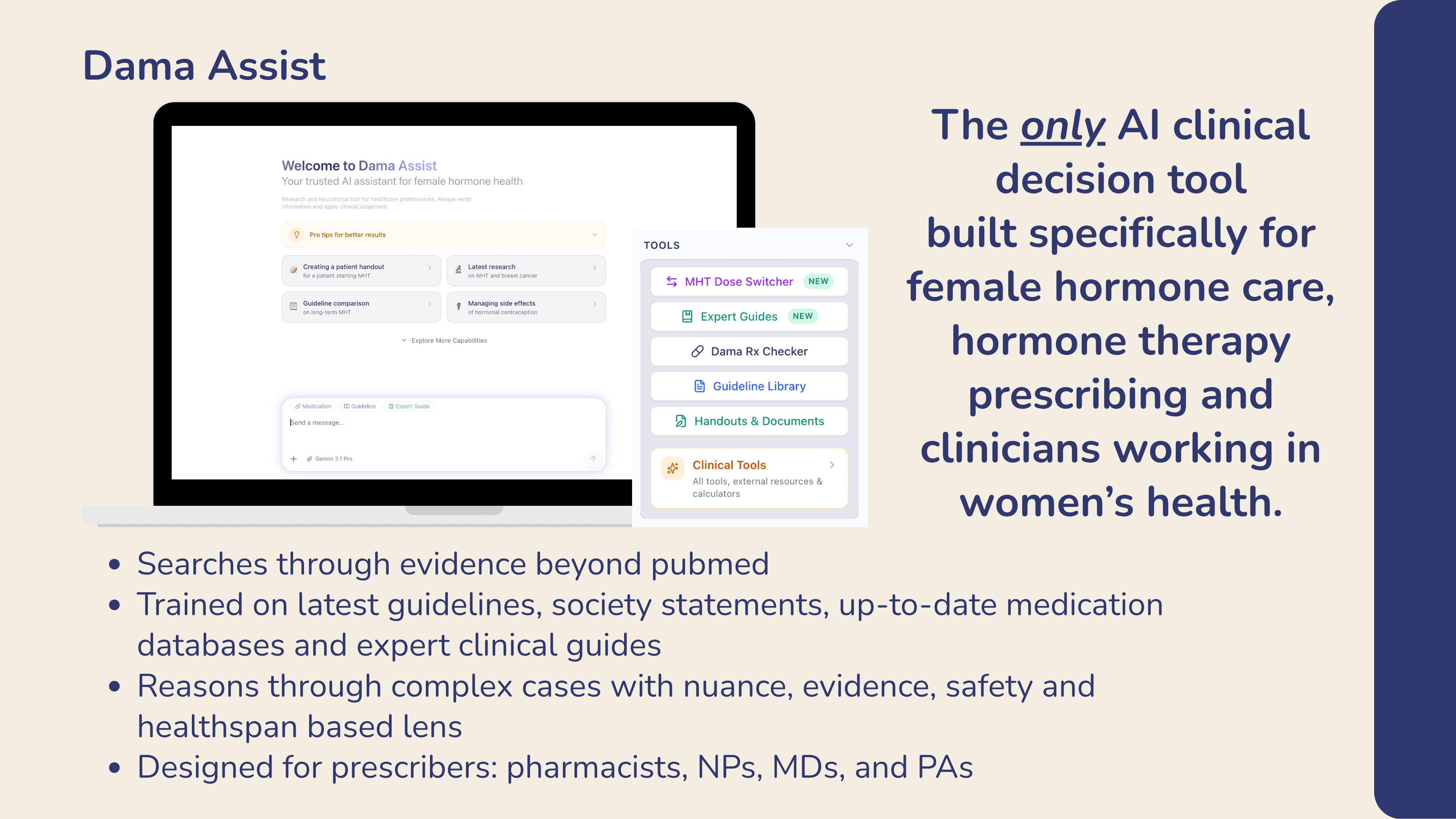
Dama Assist goes beyond synthesizing research, guidelines, and medication databases. Dama's medical expert guides, clinical consensus, and clinical decision pathways are layered in to reflect modern, personalized women's hormone care.
The Bottom Line.
While AI offers huge potential to reduce administrative burden, general AI models often lack the safety and clinical nuance required for complex areas like women’s health and hormone therapy. At Dama Health, our mission is to bridge this gap. We build evidence-based tools designed specifically for women’s health practitioners. We ensure safety, accuracy, and clinical relevance by training and testing our AI directly with women’s health experts.
We look forward to updating you on what’s new in the space next month!
Best
The Dama Health Team.